

In the ER, when a patient crashes, you have a team. You shout “Code Blue,” and six people are at your side in seconds. In Telehealth, when a patient mentions self-harm on a grainy video call, you are alone in your spare bedroom.
The silence after that call ends is deafening.
When vetting clinical mandates for major HealthTech platforms (Teladoc, Amwell, UnitedHealth), I see a hard truth: many RNs fail the transition to remote work. Not because they lack clinical skills, but because they lack “Digital Resilience.” They view remote nursing as a “retirement plan” — a break from the physical demands of the floor.
It is not a break. You trade sore feet for a creeping mental load we call “Pixel Fatigue” — and that trade is harder than most nurses expect. If you are considering this transition, you need to understand the pathology of this new role.
The Diagnosis: Why the Screen is Exhausting
Why does an 8-hour shift in a chair feel harder than a 12-hour shift on the floor? The answer lies in Cognitive Load Theory.
In a physical exam, you use all senses. You smell the alcohol on a patient’s breath, you feel the heat of a fever, you see the tremor in a hand. In Telehealth, you are stripped of your primary tactile and olfactory diagnostic tools. Your brain has to overcompensate by staring intensely at a 2D face to pick up micro-expressions.
This continuous “hyper-focus” sustains high cortisol levels for hours. By Friday, you aren’t just tired; you are suffering from Empathy Deficit. You have spent so much emotional currency trying to connect through a screen that you have nothing left for your family.
The Self-Assessment You Need Before You Apply
Most RN burnout in Telehealth is predictable. It happens to nurses who self-select into these roles for the wrong reasons. Before you update your resume, answer these four questions honestly.
1. Can you make a clinical judgment without touching the patient?
Not theoretically. Specifically. If a patient describes chest tightness on a video call and their camera quality is poor, can you build a risk picture from voice cadence, verbal description, and medical history alone — and document it with the same confidence you would after auscultation? If your honest answer is “I’d want to listen to their chest first,” remote triage may not be the right fit yet.
2. Do you self-debrief, or do you debrief out loud?
Floor nurses decompress by talking in the break room. Remote nurses do not have a break room. If your primary way of processing a hard case is venting to a colleague who was also there, you will find remote work profoundly isolating. You need a substitute: a licensed therapist, a structured peer-supervision group, or a formal employee assistance program you will actually use.
3. Is your home environment negotiable?
Not everyone has a spare room. If you share a small apartment, the “locked door” rule is not a preference — it is a clinical and legal standard. One HIPAA violation complaint from a patient who heard a family member in the background can trigger a fine ranging from $100 to $50,000 depending on the tier of negligence. That is not a scare tactic. That is the published HHS penalty structure.
4. Are you comfortable being professionally invisible?
In a hospital, your colleagues see your competence daily. In remote work, you are measured almost entirely by patient satisfaction scores and documentation throughput. If your sense of professional identity depends on being seen as a skilled nurse by the people around you, the isolation of this role will erode that identity faster than any physical fatigue ever could.
The “Sterile Field” at Home (Compliance Stress)
Beyond the mental load, there is the Compliance Paranoia. HealthTech corporations love remote models because they systematically offload the overhead of infrastructure, network security, and HIPAA compliance directly onto you. In a hospital, the IT department secures the network and the facility manager secures the doors. At home, you are the IT Director and the Compliance Officer, absorbing all the liability.
When evaluating a candidate’s readiness for these roles, I look for “Clinical Integrity.” Most fail — not because they lack intent, but because they have never been asked to audit their own home against a compliance checklist before an interview.
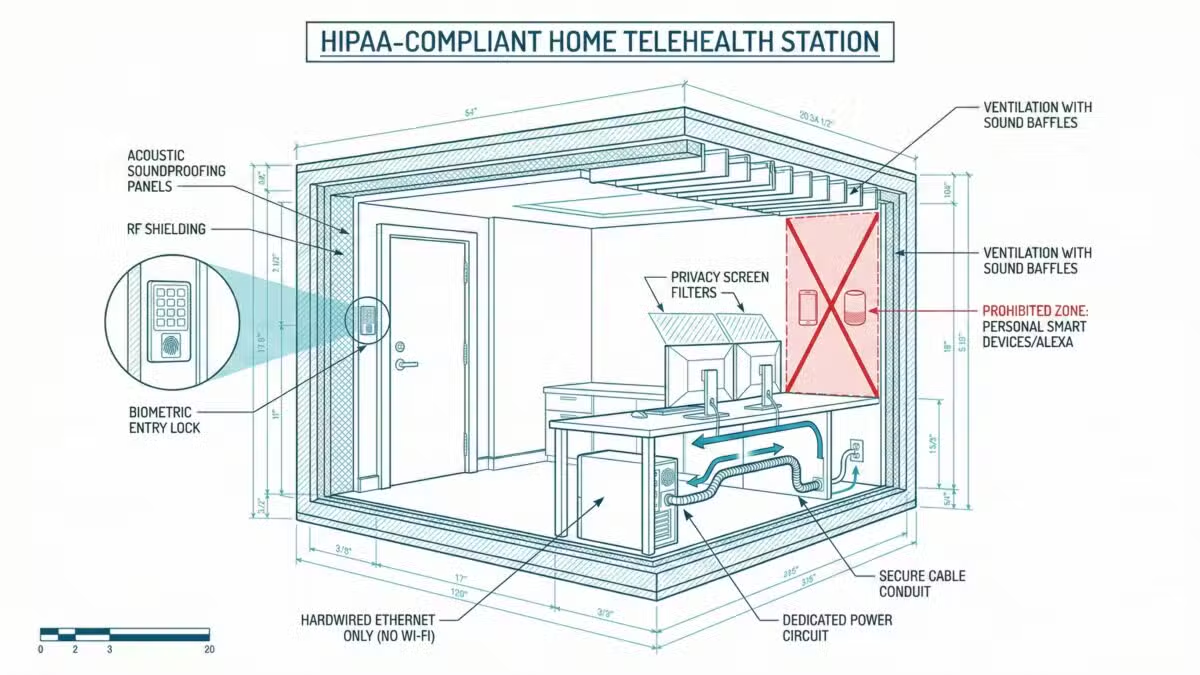
- The Window Hazard: If I see a window behind your monitor, you are a liability. Glare prevents the patient from trusting your eyes, and a passerby outside could theoretically see the patient’s data.
- The Smart Device Risk: If your Alexa or Google Home is active, you are breaching strict HIPAA Security Rules regarding ePHI. Consumer smart devices “listen,” and capturing a patient’s name without a Business Associate Agreement (BAA) is a massive compliance liability.
- The Wi-Fi Liability: Wi-Fi is unacceptable for real-time cardiac monitoring or crisis triage. If your connection drops during a suicide risk assessment, you carry the professional exposure. For premium platforms, hardwired Ethernet is a mandatory operational standard.
The Protocol: Clinical Partitioning
To survive in Telehealth without burning out, you must treat your home office like an Operating Room: a sterile zone separate from your life.
1. The Physical Partition (The Door Rule)
You cannot work from the kitchen table. You need a room with a door that locks. This is psychological as much as it is legal. When the door is closed, you are “Nurse Patel.” When the door opens, you are “Sarah.” Without this physical barrier, the emotional weight of your patients follows you out the door.
2. The Decompression Ritual
In the hospital, the commute home is your buffer. In remote work, the commute is 10 seconds. You must invent a ritual to mentally “scrub out” — the same way you would after a procedure.
My recommendation: Change your clothes. Never wear pajamas to work, even if no one sees. Wear scrubs or professional attire. At 5:00 PM, change immediately. This signals to your brain that the shift is over.
3. When the Crisis Call Comes: Your Solo Protocol
The hardest scenario in Telehealth is not a missed diagnosis. It is a patient who mentions self-harm — and you are the only person on that call. Most RNs freeze in this moment, not from lack of training, but because every crisis protocol they learned was designed for a room with backup. Here is what that call actually looks like, and what you do.
Phase 1 — Anchor the connection (first 90 seconds). Your instinct will be to reach for your documentation system. Resist it. Eye contact through the camera is your only lifeline right now. Move your notes app to a second screen or a notepad beside you before your shift starts. Use these exact words: “I hear you. I’m not going anywhere, and I’m not going to rush you.” The patient does not need a protocol in this moment. They need proof that you are present.
Phase 2 — Assess and loop in silently. While keeping the patient talking, use your platform’s internal escalation channel — not a phone call that forces you to look away or put the patient on hold. Most major platforms (Teladoc, Amwell) have a supervisor alert that is a single keystroke. Know exactly where that key is before your first shift. If your platform does not have one, raise that during onboarding. A platform that routes you into crisis calls without a silent escalation path is not a partner. It is a liability.
Phase 3 — The mandatory debrief. After any mental health crisis call, you are not cleared for your next appointment in eight minutes. Document the interaction, then send a direct message to your supervisor flagging that you need a 15-minute buffer before resuming. If your employer has no policy for post-crisis recovery time, put the request in writing. You are creating a paper trail that protects your license if the case is ever reviewed.
The Final Prognosis: Operational Discipline
The nurse who thrives in Telehealth is not the one who misses the hospital least. It is the one who builds a new clinical environment just as deliberately as she built her skills — locked door, hardwired cable, debrief ritual, and all.
If you treat this role with the same clinical rigor you would an ICU shift, you can have a long, sustainable career. If you treat it like a paid vacation, you will be a casualty of the new digital burnout.
The One Investment That Protects Everything
Every compliance item in this article — the Ethernet cable, the locked door, the privacy screen — is meaningless without one additional layer: professional liability insurance you own independently of your employer.
Telehealth platforms classify most remote nurses as W-2 employees, which technically places you under their malpractice umbrella. But that coverage protects the platform’s interests, not yours. If a crisis call goes wrong and the platform’s legal team decides the documentation was insufficient, you need counsel that answers to you — not to their risk management department.
Independent nursing malpractice coverage costs $100–$300 per year. It is the cheapest thing in your entire remote setup, and the most important one. Before you sign any Telehealth employment contract, confirm two things: what the platform’s coverage limit is, and whether you are individually named on the policy or just covered as an employee of the entity. Those are different things. A benefits coordinator who cannot answer that question clearly is a red flag.




